Table Of Content

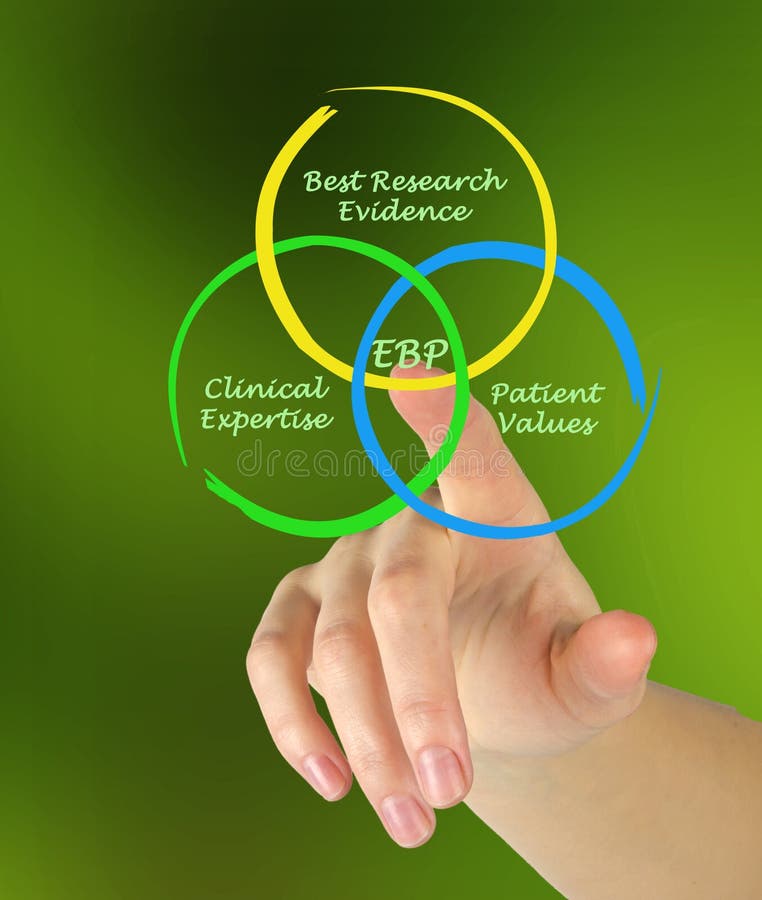
The process of collecting occupant and management perspectives as well as objective environmental and human productivity and health data to enable design decision making based on credible research to achieve the best possible outcomes. The offices sector has been widely studied with the major concerns focusing on productivity. A study in 2000 by Sheffield Hallam University[36] reported that apart from surveys of occupants of individual offices, the evidence base on new workplaces was mainly journalistic and biased towards interviews with successes and failures. Some companies claimed that new spatial arrangements led to reduced costs, reduced absenteeism and easier recruitment, faster development of new ideas, and increased profitability.
Patient Satisfaction
Following our EBM-SDM course, not only did junior doctors’ knowledge and skills improve, but they frequently referred to the benefits of including patients in their discussions about care, which indicated that they had expanded their understanding of EBM to incorporate aspects of person-centered care. Their intentions to be more person-centered were frequently based on using evidence to effectively communicate risks and benefits to patients, rather than having SDM conversations with patients where all options were described, and decisions made together. However, there appeared to be a disconnect between the practice of SDM and the recognition of its practice. On several occasions, junior doctors facilitated SDM by answering patient questions after the consultant left the room, or by reiterating what the consultant said, but failed to recognise this as part of a SDM conversation with the patient. Consultants varied greatly in their understanding of EBM and SDM, and their views on whether either should be practised by junior doctors. Senior consultants who completed medical training before the formal introduction of EBM in the 1990s [39] appeared to be unfamiliar with and less accepting of EBM and SDM and expressed a reluctance for junior doctors to engage in either.
Design for Emergency Management - Faculty Books - The Voice of Wilkinson - Chapman University
Design for Emergency Management - Faculty Books - The Voice of Wilkinson.
Posted: Mon, 11 Sep 2023 07:00:00 GMT [source]
Other Literature Sources
Of the 12 participating junior doctors, five were fellows, five were registrars, one was a resident, and one was an intern, and thus the junior doctor cohort represented a range of training levels and experience. Half of the junior doctors undertook their medical training in Australia and around two-thirds had some prior EBM instruction, although none had received training in SDM. Five junior doctors completed both pre and post interviews; those who only completed one interview cited time factors and clinical schedules as reasons for non-completion. Most junior doctors who completed the EBM-SDM training course but not the interviews cited time factors as reasons for their non-participation. As EBD is supported by research, many healthcare organizations are adopting its principles with the guidance of evidence-based designers.
Process
Become EDAC certified to gain in-depth knowledge of evidence-based design and become part of a global community of forward thinkers who envision a world where all environments are created using evidence-based design. Performative spaces must now be designed to evolve as rapidly as the needs of those that occupy them. This new publication provides detailed design strategies, case studies and the latest advances in the use of new technologies to illustrate the ways in which evidence can be integrated into the design process.
A state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity. Do the physical properties of an exhibition space and the hanging of artworks affect the viewing behaviour of visitors? To answer this and other significant questions, a series of experiments were conducted in the St. Gallen Fine Art Museum in Switzerland.

Iterative generation of codes and themes took place with other members of the authorship team (FR, YZ, LAE, GF, SS). Themes were inductively defined as new codes were generated and all themes and sub-themes were named. Transcripts were re-read, and themes reinterpreted until the team decided that data findings had been accurately described. These themes were then used in Phase 2 of the study as a framework to deductively analyse consultants’ interviews.
Improving the Health Care Environment and Processes
In the higher education sector, a review by CABE[35] reports on the links between building design and the recruitment, retention and performance of staff and students. A demographic survey was developed by four authors (MSi, FR, YZ, AD) and emailed to all consenting participants to record their age group, gender, position, country of medical training, period in which training occurred, and prior education in EBM and SDM. Bringing together individuals and groups to share, learn, and advocate for ideas and practices that advance the impact of healthcare design. Identifying the evidence and impact that facility design makes for patients, staff, families, and the bottom line. At HMC Architects, we believe a successful design is one that ultimately enriches the lives of patients, families, healthcare professionals, and communities. Establishing a vision that defines the goals and objectives for evidence-based design is the most important step.
Arrangements that promote social interaction in waiting areas include comfortable, supportive furniture positioned in small, flexible groupings, with seating placed at right angles. Large dining areas should be subdivided with tables seating four to encourage social interaction, enhance relative privacy, and improve eating behavior. Light.Bright light, either natural or artificial, can improve patient outcomes, affecting such factors as depression, agitation, sleep, circadian rest/activity rhythms, and length of stay. Sunlight has been linked with shorter stays, lower stress, less pain, lower intake of pain medication, and even lower mortality. For staff, ensuring that appropriate, nonglare light levels are brought to the tasks at hand can improve staff accuracy and effectiveness.
Healing Environment
Working closely with our clients, we ensure that project goals are met while delivering designs that benefit the people who live, work, and interact in these spaces. The video presents the experiences of three model hospitals—Griffin Hospital in Derby, CT; Holy Cross Hospital in Silver Spring, MD; and Woodwinds Health Campus in Woodbury, MN—that incorporated evidence-based design elements into their construction and renovation projects. As an approach to design, PBBD tries to create clear statistical relationships between design decisions and satisfaction levels demonstrated by the building systems. Like EBD, PBBD uses research evidence to predict performance related to design decisions. When we partnered with Torrance Memorial Medical Center administrators to create a new hospital tower, we researched and implemented design elements that support the best patient experiences.
Additionally, interviewing healthcare professionals and surveying patients can provide valuable information and insights that studies don’t. For example, research may show that many patients with mobility issues prefer to press a button from bed to call for assistance from staff instead of getting out of bed to seek help, which could be unsafe. However, anecdotal evidence provided by nursing staff may point out that while patients say they want such a convenient and safe call feature, many will try to walk on their own to find assistance. That observation might lead you to design your hospital rooms to accommodate both types of patients. Installing call buttons as well as handrails along the bedside walls of patient rooms can lower the risk of injury. Because of this, it’s important to understand how the built environment can be part of the overall strategy to improve health outcomes and minimize hospital errors and omissions to create a safe, effective, efficient, and equitable setting for the treatment of patients and for the families that support them.
MSi knew all study participants (except two consultants) through her work as a clinical librarian at Macquarie University and discussed with the other authors how her involvement in the study and familiarity with the participants may influence her perceptions and analysis of the interview data. FR, YZ, and SS are health service researchers, with extensive experience in qualitative research. As non-clinicians, they reflected on their experiences and expectations as patients, and as researchers, and how that may influence their interpretation of the interview data.







No comments:
Post a Comment